46 Y/O female:- Status epileptics ; CKD
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
CASE
This is a case of 46 y/o female, admitted in ICU with the complaints of:-
- 2 episodes of involuntary movements of upper and lower limbs and hemoptysis on 31st December 2022
History of Presenting Illness:-
Pt. Was apparently asymptomatic 13 years ago,
Then she developed pain in lower back region and generalised weakness for which she went to local hospital.
Then during routine investigations she was found to have elevated creatinine, and was started on conservative management .
Since then ,she is on routine follow+up with hemogram and serum creatinine levels,and her baseline creatinine levels were 3.2mg/dL.
In june 2022,she developed fever and productive cough associated with SOB for which CT chest was done,showing peripheral ground glass opacities,and septal thickening was noted
After a few days, she also developed swelling of both lower limbs ( till ankle joint) which were insidious in onset and gradually progressive
Then she underwent dialysis for the first time.
3 months later, she developed fluid filled bleb, on one finger and then over all the 10 fingers of hand got involved in a span of 10 days. Some of this blebs ruptured on their own and some were pricked by the patient.
She developed eroding and distorted nails , hyperpigmented macules over the face and itching over the palms,and low grade fever associated with loss of apetite and alopecia.
Ulcers over palms , pulp of fingers associated with burning sensation
With autoimmune etiology suspicion, she was investigated further and was ANA profile and was tested Positive for Anti Ro 52and SSA/Ro 60++,and SSB/La+.



In view of the persistent low Hb 5-6g/dL,bone marrow aspiration (from right posterior iliac spine)was done for evaluation of anemia.
Then she was started on mycophenolate mofetil 360mg,and later was planned to shift to cyclophosphamide as she is not responding to MMF.( But was not started in view of renal insufficiency).
SHE WAS PUT ON MYCOPHENALATE MOFETIL, HYDROXYCHLOROQUINE , OMNICORTIL
In November she developed cough since 1 week,with whitish color sputum which is mucoid in consistency and moderate in amount and non blood stained and non foul smelling .
Bilateral swelling of lower limbs till knee,not associated with trauma,and decreased urine output for 2 days,and Shortness of breath( MMRC grade 3),and loss of appetite.
Then ,she was diagnosed as
*?Antisynthetase syndrome
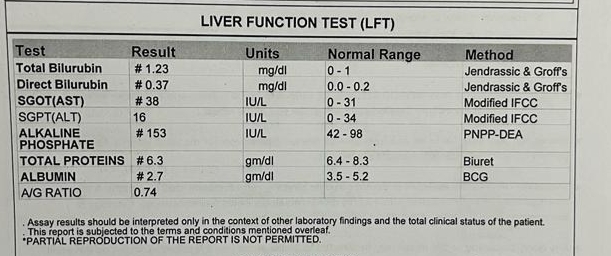
*CLD secondary to autoimmune hepatitis with hypoalbuminemia *
acute exacerbation of ILD
*recurrent anemia
She did not develop any new skin lesions,oral ulcers.
In December,she was taken to another hospital
Due to increase in the SOB with abdominal distension ,
Then she was taken to second session of dialysis.
Her antibody profile was repeated.

Skin biopsy was done

Bronchoalveolar lavage was performed and was found to be having an infective etiology and mucus plugs in the airways.

On ultrasonography,hypoechoic lesions were found in the liver, PET CT was advised and was done.


So they suspected infective etiology probably TUBERCULOSIS,and started her on antitubercular therapy
Tab ISONIAZID 300mg daily
Tab RIFAMPICIN 500 mg OD daily
Tab PYRAZINAMIDE 1500 mg thrice a week
Tab ETHAMBUTOL 1200 mg thrice a week
,since 20 days.( But afb, genexpert are all negative)
CURRENT PRESENTATION
2days back she developed sudden onset movements of UL and lowerlimbs, for 3-4 minutes, associated with blood from mouth,and there is a brief period of LOC .
similar episode one at 6:00 am, and then 2 similar episodes after they came here at 8:00am.
At presentation her blood pressure was 170/110 mmhg
Source:- colleagues
Her seizures continued each episode about 2 mins and post ictal confusion was present.
In view of recurrent seizures CT brain was done.
inj lorazepam was given,
later leviteracetam and
when her seizures weren’t controlled then sodium valproate was given
She later then had continuous episodes of seizures lasting for more than 45 minutes .
In view of respiratory distress ( sats 60 ),and uncontrollable recurrent seizures she was sedated with IV MIDAZOLAM and intubated.
Post intubation, she had cardiac arrest ( no central pulses palpable ) 2 cycles of CPR done ROSC was achieved .
GENERAL EXAMINATION
Patient is in sedation.
She has hyperpigmentation on the face, upper limbs


Her nails





Single Bleb on the right hand
VITALS:
Temperature:afebrile
BP 160/110mmhg
Pulse 158bpm
RR 37 cpm
SYSTEMIC EXAMINATION
CVS : S1,S2 heard. No murmurs
RS : Bilateral air entry present
Normal vesicular breath sounds were heard
CNS
Meningeal signs were absent
Pupils: mid dilated , reactive to light
DOLL'S EYE
Reflexes:
SUPERFICIAL:
CORNEAL REFLEX present
CONJUNCTIVAL REFLEX present
DEEP TENDON REFLEXES:
Rt. Lt
Biceps: 2+ 2+
Triceps 2+. 2+
Supinator. A. A
Knee. A. A
Ankle A. A
PROVISIONAL DIAGNOSIS:
STATUS EPILEPTICUS, (seizures secondary to hemorrhagic stroke
?autoimmune vasculitis
? Metabolic cause( increased urea)
Investigations
ON DAY 1

MRI diagnosis : POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME.







Day 2





On 04-01-2023:




As on 6/01/23










Comments
Post a Comment